This question was presented two weeks ago in poster format at the annual European Academy of Neurology conference in Vienna, Austria. The title can be cited as: Roesel T. Do “Havana Syndrome” and Gulf War Illness Share Neuroinflammation as a Common Disease Mechanism? European Journal of Neurology 2022. 29 (Supplement 1): 870.
The abstract reads:
Introduction
Multiple neurological symptoms reported by North Americans following deployment exposures characterize Gulf War Illness (GWI) and “Havana Syndrome” (HS). MRI-detected brain structural alterations are present in both but with disparities. Integrated PET/MRI scans, using the radiolabel 11C-PBR28 (peripheral-type benzodiazepine receptor), detects neuroinflammation by binding to upregulated translocator proteins (TSPO) in activated astrocytes and microglia. Significant neuroinflammation in the precuneus (PC), dorsolateral prefrontal (dlPFC) and middle anterior cingulate cortex (mACC) areas was so demonstrated in 15 GWI veterans (Alshelh, et al., Brain Behav Immun, 2020). Since neuroinflammation has yet to be documented for HS, the feasibility of a PET/MRI TSPO study is determined herein.
Methods
Adjusted standard uptake volume ratio (SUVR) values for the 25 normal controls referenced above was provided by Dr. Alshelh. Sample size calculations to achieve t-tests with powers greater than 0.8 were performed to assess feasibility. Constraints were Type I error of 0.05 and a patient-control allocation of 1:1. Subtraction of the SUVR control means from the SUVR GWI means for the PC, dlPFC, and mACC areas, derived the clinically significant SUVR delta values of 0.050, 0.048, and 0.054, respectively.
Results
Twenty-two HS patients and 22 normal controls suffice to construct a TSPO neuroinflammation study with adequate power.
Conclusion
An HS TPSO integrated PET/MRI study of 44 subjects is feasible. If HS neuroinflammation is revealed, new insights can be attained into HS pathophysiology and its potential etiology. Furthermore, preventive or treatment measures for one illness may apply to the other.
Addendum: A thank you goes out to Dr. Alshelh for sharing the adjusted standard uptake volume ratios acquired from the 25 normal civilian controls. These were published in the Brain, Behavior, and Immunity article referenced above. These values made the statistical calculations possible. The 25 normal civilian controls without military service history are thanked as well for their participation in a study that benefits previously deployed service members. Dr. Alshelh’s work can also be seen in a You Tube video summary at: https://www.youtube.com/watch?v=eOiFoKD8j_E
A recent article in the Journal of Clinical Epidemiology referenced in Nature (Many researchers say they’ll share data — but don’t (nature.com)) reminds us that few authors (7%) actually respond to data requests, so additional thanks to Dr. Alshelh is in order!
CERVOE.org seeks partners to further the understanding of health risks and develop treatment options for deployment related illnesses.
Prior CERVOE.org posts have detailed how isosorbide dinitrate (ISDN) may have anti-SARS-Cov-2 activity. These ideas are being presented at a meeting expressly dedicated to drug discovery for cardiopulmonary diseases including COVID. The poster presented at the American Heart Association last November will be presented again on Tuesday, May 24 with updated information. Although oral ISDN is available in the U.S. for cardiac angina, an intravenous (IV) formulation has not been FDA approved. In contrast, most countries in the world have IV ISDN listed in their national formulary. CERVOE.org is seeking partners to launch a pilot study through a clinical trial platform to investigate IV ISDN as a COVID drug, after an investigational new drug (IND) application with the FDA has been approved. Another drug option to treat hypoxia and complications of moderate to severe COVID offers the opportunity to save a life, whether that of civilian or a service member infected with SARS-CoV-2.
This is the title of the poster abstract that was presented at the 2021 American Heart Association Scientific Sessions virtual meeting last month with the support of CERVOE.org. A successful randomized clinical trial would demonstrate that isosorbide dinitrate can help this cohort of COVID patients that have a very high mortality. It would also add to the evidence that isosorbide dinitrate has anti-viral properties by inactivation of the SARS-CoV-2 main protease (Mpro). S-nitrosylation of cysteine 145 in the active catalytic site is the posited mechanism of action.
The abstract for poster@9991 can be found at:
https://www.ahajournals.org/doi/abs/10.1161/circ.144.suppl_1.9991
Any citation should read: Roesel, T. Can Isosorbide Dinitrate Save Lives in Hospitalized COVID-19 Patients with Hypertension and a Defined Cardiac Injury? Circulation. 2021;144 (supplement):A9991
A copy of the abstract and figure as it appears in the above reference follows:
Abstract 9991: Can Isosorbide Dinitrate Save Lives of Hospitalized COVID Patients with Hypertension and a Defined Cardiac Injury?
Originally published 8 Nov 2021Circulation. 2021;144:A9991
Abstract
Introduction: As defined by MB-CPK, hsTn-I, MB, or EKG and/or cardiac echo abnormalities, cardiac injury (CI) determines a median survival time (MST) of 10 days for hospitalized COVID patients (HCPs). HCPs without defined CI have an MST beyond 39 days (Huang, et al., see Figure). Hypertension (HTN) presents in 17-41% of HCPs in various studies, with COVID mortality independent of HTN. Therefore, a randomized clinical trial (RCT) is proposed for HCPs with CI and incidental BP elevation to compare IV isosorbide dinitrate (ISDN) with usual anti-HTN care (UC). Vasodilatory ISDN lowers BP, and has been proposed as an anti-SARS-CoV-2 drug. Others report improved survival of ISDN treated Coxsackie B3 virus-infected mice as evidence for anti-viral activity. The endpoint for this CI RCT pilot of 100 ISDN-treat HCPs and 100 UC controls is mortality. Secondary endpoints are interval biomarkers to dissect ISDN anti-viral action.
Methods: Log-rank analysis was performed with 1:1 allocation. Accrual time was 180 days with a 60-day follow-up. Power was 0.8 with a type I error of 0.05.
Results: For 200 total subjects, an MST greater than 14.9 days in the ISDN arm was significant if UC stays at 10 days (see Figure).
Conclusions: Testing repurposed ISDN as a COVID drug is feasible. A successful pilot with improved MST suggests ISDN has anti-SARS-CoV-2 action, since COVID mortality is independent of HTN. Biomarkers could include viral clearance, oxygenation, D-dimer, IL-6, LDH, as well as platelet and lymphocyte counts. The need to treat HCPs with elevated BP per guidelines permits study entry. Cross-over treatment occurs if a regimen fails. Immunomodulators and remdesivir are administered per COVID treatment guidelines for all HCPs. IV ISDN, bolused and/or infused, avoids 1st pass hepatic effects. IV IDSN is approved in most countries, but not in the USA or Canada. A successful pilot would permit larger IV ISDN RCTs as IND RCTs, and can serve as a template for other treatments for HCPs with defined CI.

Recruitment for the clinical trial titled “SARS-COV-2-Spike-Ferritin-Nanoparticle (SpFN) Vaccine With ALFQ Adjuvant for Prevention of COVID-19 in Healthy Adults (NCT04784767)” has been halted, yet the study status remains active per ClinicalTrials.gov. An Army bulletin states that a soon-to-be completed analysis will provide information on the effectiveness of SpFN in humans. This data will permit the comparison of SpFN with other emergency-use authorized COVID vaccines. A thank you goes out to all of the civilian volunteers.
The bulletin can be viewed at:
The advantage of SpFN over the other COVID vaccines is that it can provide a ferritin-based scaffold to target current and future protein targets of SARS-CoV-2 variants, as well as other coronaviruses.
Walter Reed Army Institute of Research (WRAIR) is seeking 72 volunteers for inoculation of a new investigational COVID-19 vaccine at its Silver Spring, Maryland Clincal Trials Center (CTC) site. Paul Scott, MD, MPH is the principal investigator. The study started on April 5, 2021. The new vaccine is constructed from ferritin nanoparticles to which the spike protein from the SARS-CoV-2 coronavirus is attached. The vaccine is called the spike ferritin nanoparticle (SpFN) COVID vaccine and carries the FDA determined investigational new drug identifier IND 27301. The study has the WRAIR research number 2847, which is registered as a study with ClinicialTrials.gov as NCT04784767.
The phone contact is 866-428-2788.
Email contact is: usarmy.detrick.medcom-usamru-w.mbx.clinical-trials@mail.mil
There are many criteria that need to be met to participate. These conditions are outlined at the above CTC website. The key criteria are that non-military participants need to be male or female (not pregnant or breastfeeding), aged 18-55, without autoimmune disease or diabetes and testing negative for COVID. An individual needs to be available to the CTC in Silver Spring for 12 months after inoculation of two study vaccine doses. Those who have not had a prior COVID vaccine are only eligible to participate.
Why does the military need non-military volunteers? Service members are not permitted to participate as they are an ethically protected group, because they do not have autonomy.
Why does the military need another vaccine other than the ones currently available to the public? The military is concerned about service members who may be deployed in the future to areas where a new coronavirus or virus strain has emerged. The current vaccines may offer no protection in those circumstances. The SpFN COVID vaccine can be more easily manipulated to accommodate any such new coronavirus to achieve the required protection. The military needs to maintain a posture of readiness should deployments occur to an area with an emerging infecxtious disease.
This notice is for informational purposes only and does not constitute a recommendation by CERVOE.org. Any study participation is based on the decision between the participant, his or her physician, and the principal investigator. Any unintended consequences from participation is solely the responsibility of the aforementioned parties. CERVOE.org makes no recommendation for an individual to participate.
There are some interesting videos which show the CTC and an interview with the first participant. They can be found at:
Tour of the CTC:
https://www.dvidshub.net/video/789722/wrair-starts-phase-trials-new-covid-19-vaccine
First Participant Interview:
Poster Presentation at the American Society of Clinical Pharmacology and Therapeutics March 8 — March 17, 2021
Deployed service members are at risk now and in the future to current and new coronavirus strains. This is evident by outbreaks onboard the USS Theodore Roosevelt, USS San Diego, and USS Philippine Sea. Better treatments to prevent mortality are needed should vaccines be ineffective against new coronavirus strains. The following abstract and poster on isosorbide dinitrate as a repurposed drug addresses this need. CERVOE.org is promoting future trials of isosorbide dinitrate as a COVID-19 treatment through various efforts. Partners are invited to join in this endeavor. Contact info@cervoe.org.
To view an enlarged poster version, click on the poster overlay below:

Copyright 2021 Thomas R. Roesel
The following abstract for this poster has been published in Clinical Pharmacology and Therapeutics. The citation should read: Roesel, T. Clinical Trial Design to Test Isosorbide Dinitrate as an Anti-Viral Treatment for COVID-19. Clinical Pharmacology and Therapeutics 2021, 109 (S1):47. It can be found at https://doi.org/10.1002/cpt.2167 by scrolling halfway down the list of posters. It is identified as poster PIII-009 and reads as follows:
CLINICAL TRIAL DESIGN TO TEST ISOSORBIDE DINITRATE AS AN ANTI-VIRAL TREATMENT FOR COVID-19
T. Roesel; CERVOE.org, Bozman, MD, USA.
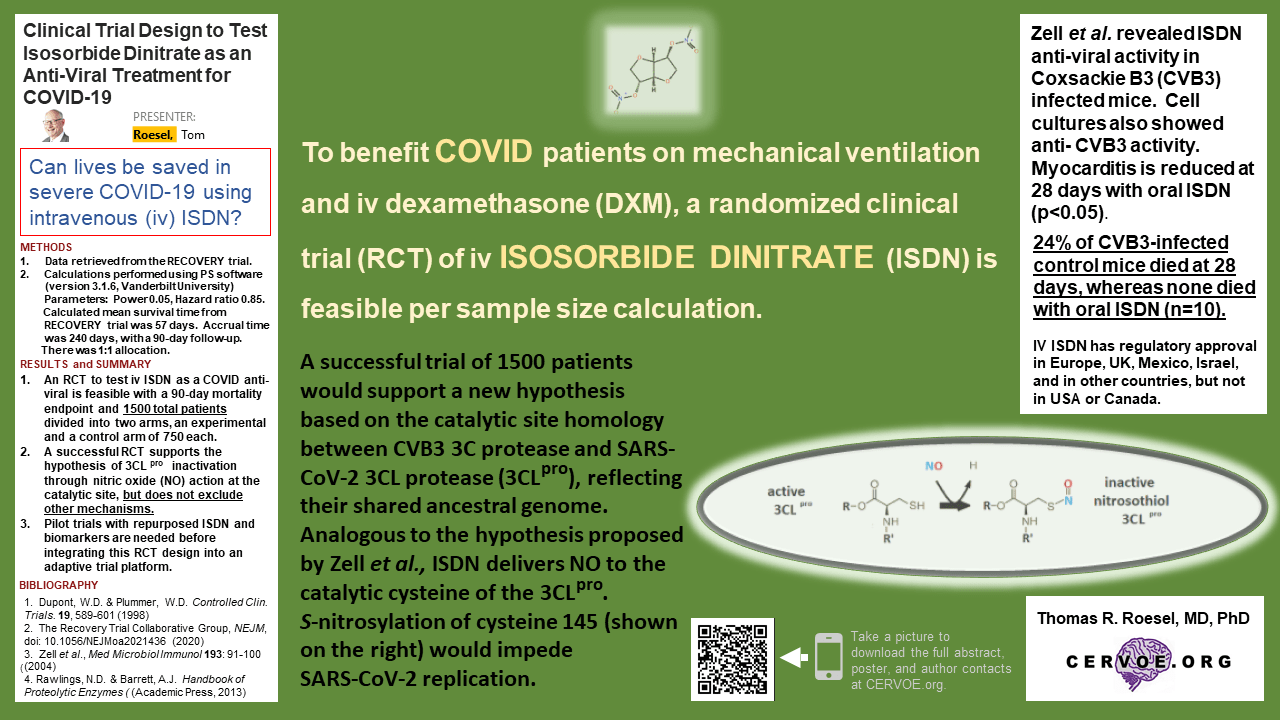
BACKGROUND: COVID-19 is characterized by pulmonary disease that can lead to death. In the RECOVERY trial (1), those infected and intubated who received dexamethasone (DXM) for 3 to 10-days (6 mg/day), had an improved 28-day mortality of 29.3% vs. 41.4% for control (RR of 0.64, 95% CI 0.51 to 0.81). ClinicalTrials.gov lists several COVID randomized clinical trials (RCTs) testing nitric oxide (NO) gas, but none use NO donor isosorbide dinitrate (ISDN). Since ISDN antiviral activity was shown in vitro and in Coxsackie B3 virus (CVB3) infected mice (2), an RCT using ISDN vs. placebo is proposed for intubated COVID patients who receive 10-days of DXM concomitantly.
METHODS: Log-rank analysis determined sample size for RCT feasibility. Accrual time was 240 days with 90-day follow-up. Placebo to drug allocation was 1:1. Power was 0.85, and type I error was 0.05. A calculated median survival time for those intubated and on DXM was derived from the RECOVERY trial. The RR ratio of 0.85 was deemed significant. All subjects would receive 10days of DXM with either 10days of placebo or IDSN.
RESULTS: Calculations reveal that an RCT with a 28 day mortality end-point requires 1492 patients, divided between 746 experimental subjects and 746 controls.
CONCLUSION: An RCT pitting repurposed ISDN against placebo to treat COVID is feasible. A positive ISDN RCT in DXM-treated COVID patients would then warrant evaluation in non-intubated patients. ISDN enhances O2-release from oxyhemoglobin in vitro under low O2, a possible benefit for hypoxic patients. Others postulate that NO inactivates the catalytic cysteine 147 residue of the CVB3 3C protease as the mechanism of antiviral ISDN action. Based on catalytic site homology between the SARS-CoV-2 3CLpro (Mpro) and CVB3 3C protease, one could infer a shared mechanism.
1. The RECOVERY Collaborative Group. Dexamethasone in Hospitalized Patients with Covid-19 — Preliminary Report. New England Journal of Medicine 2020. doi: 10.1056/NEJMoa2021436.
2. Zell, R., et al. Nitric oxide donors inhibit the Coxsackievirus B3 proteinases 2A and 3C in vitro, virus production in cells, and signs of myocarditis in virus-infected mice. Med. Microbiol. Immunol. 193, 91:100 (2004).
CERVOE.org seeks to promote clinical trials among civilian participants who value the commitment that service members make in serving their country. Some people are aware that there are particular risks directed to soldiers, sailors, guardians, airmen and airwomen, that are unique to their deployments. Not all of these risks are known when service members deploy. Unforeseeable deployment-related health impairments are not recognized until after their return. More often than not, post-deployment studies on veterans reveal medical insights that later benefit civilians.
Many are not aware that ethical constraints prevent many military-related health investigations. Service members are protected from coercion in this manner. Therefore, some anticipated military-related medical questions are difficult to study. By seeking to highlight specific clinical studies, which ask medical questions in the civilian world, yet benefit service members, CERVOE.org hopes to improve the health of those who go in harm’s way. This is an addition to the mission of CERVOE.org that centered on establishing a disease-specific cerebral endothelial cell repository. The goal of this organization now includes encouraging civilian participation in clinical trials that help our service members. Posts hereafter will reflect this new mission.
Envisioned are the development of computer chips that modulate the central nervous system in a closed loop manner to improve the mental and physical health of military personnel after deployment. ElectRx, pronounced as “electrics” refers to an electrical rather than a drug prescription.
The announcement can be found it the following link:
As quoted in the link above: “…the Defense Advanced Research Projects Agency (DARPA) is announcing a new $78.9 million research program to develop minimally-invasive neurotechnologies that may help treat many diseases, including PTSD. In addition, the White House announced that this fall it will host the White House BRAIN conference, including a focus on PTSD and TBI.”
The DARPA announcement can be found in the next link that follows:
http://www.darpa.mil/NewsEvents/Releases/2014/08/26.aspx
As stated by Doug Weber, DARPA program manager in the above link: “Instead of relying only on medication—we envision a closed-loop system that would work in concept like a tiny, intelligent pacemaker. It would continually assess conditions and provide stimulus patterns tailored to help maintain healthy organ function, helping patients get healthy and stay healthy using their body’s own systems.” The website goes on to state that ElectRx seeks to create ultraminiaturized devices, approximately the same size as individual nerve fibers, which would require only minimally invasive insertion procedures such as injectable delivery through a needle.
Cervoe seeks to support research that builds on known findings from transcranial direct current stimulation, transcranial magnetic stimulation, and electroacupuncture, all minimally invasive techniques that alter central nervous system function, to attain the same goals as ElectRx.
The U.S. Defense Advanced Research Projects Agency (DARPA) announces the Systems-Based Neurotechnology for Emerging Therapies (SUBNETS) program for competitive grants. The grants encourage developing concurrent brain stimulation and monitoring technologies that treat and monitor a variety of brain illnesses. Targets of the grant are traumatic brain injury (TBI), post–traumatic stress disorder (PTSD), depression, anxiety, personality disorders, substance abuse, addiction, fibromyalgia, and chronic pain. Technologies are sought that restore brain function through multi-region recording and stimulation, whereby neural dysfunction, associated with behavioral abnormalities, can be observed and an intervention through neural actuation is applied. DARPA wishes to promote research on technologies that create closed-loop diagnostic and therapeutic systems. These technologies can lead to better modeling and understanding of the relationship between neural systems and behavior, as well as better therapies for brain diseases. Cervoe sees overlap of these goals with its own commitment to promote research in non-invasive transcranial direct current as well as magnetic brain stimulation (tDCS and TMS). A desired closed-loop diagnostic and therapeutic system is created when such non-invasive techniques are paired with newer gadolinium functional magnetic resonance (fMRI) imaging techniques that assess blood brain barrier (BBB) dysfunction in TBI and neurodegenerative diseases.
For access to the 49 page DARPA announcement describing SUBNETS as a pdf file go to:
https://www.fbo.gov/utils/view?id=630c11c6f54ac0696bcba2e2cb014efb
For more on gadolinium fMRI assessment of the BBB function, go to the Chassidim et al. article that recently appeared in Fluids and Barriers of the CNS titled “Quantitative imaging assessment of blood-brain barrier permeability in humans.” This article is found at: http://www.fluidsbarrierscns.com/content/10/1/9